The Medical Council of India (MCI) has seen a few major controversies over the past decade. In the latest incident, MCI President, Dr. Ketan Desai was arrested by the CBI on charges of accepting a bribe for granting recognition to Gyan Sagar Medical College in Punjab. Following this incident, the central government promulgated an ordinance dissolving the MCI and replacing it with a centrally nominated seven member board. The ordinance requires MCI to be re-constituted within one year of its dissolution in accordance with the provisions of the original Act. Background The Medical Council of India was first established in 1934 under the Indian Medical Council Act, 1933. This Act was repealed and replaced with a new Act in 1956. Under the 1956 Act, the objectives of MCI include:
Over the years, several committees, the most recent being the National Knowledge Commission (NKC) and the Yashpal Committee, have commented on the need for reforms in medical regulation in the country. The Ministry of Health and Family Welfare (MoH&FW) has recently released a draft of the National Council for Human Resources in Health (NCHRH) Bill for public feedback. (See http://mohfw.nic.in/nchrc-health.htm) Key issues in Medical Regulation Oversight Currently, separate regulatory bodies oversee the different healthcare disciplines. These include the Medical Council of India, the Indian Nursing Council, the Dental Council of India, the Rehabilitation Council of India and the Pharmacy Council of India. Each Council regulates both education and professional practice within its domain. The draft NCHRH Bill proposes to create an overarching body to subsume these councils into a single structure. This new body, christened the National Council for Human Resources in Health (NCHRH) is expected to encourage cross connectivity across these different health-care disciplines. Role of Councils Both the NKC and the Yashpal Committee make a case for separating regulation of medical education from that of profession. It is recommended that the current councils be divested of their education responsibilities and that these work solely towards regulation of professionals – prescribing a code of ethics, ensuring compliance, and facilitating continued medical education. In addition, it has been recommended that a national exit level examination be conducted. This exit examination should then serve the purpose of ‘occupational licensing’, unlike the prevalent registration system that automatically grants practice rights to graduating professionals. In effect, it is envisaged that the system be reconfigured on the lines of the Institute of Chartered Accountants, wherein the council restricts itself to regulating the profession, but has an indirect say in education through its requirements on the exit examination. A common national examination is also expected to ensure uniformity in quality across the country. Both committees also recommend enlisting independent accrediting agencies for periodically evaluating medical colleges on pre-defined criteria and making this information available to the public (including students). This is expected to bring more transparency into the system. Supervision of education – HRD vs. H&FW The Ministry of Human Resources and Development (MHRD) is proposing a National Council for Higher Education and Research (NCHER) to regulate all university education. However, MoH&FW is of the opinion that Medical Education is a specialized field and needs focused attention, and hence should be regulated separately. However, it is worth noting that both the NKC and the Yashpal Committee recommend transferring education overseeing responsibilities to the NCHER. Internationally, different models exist across countries. In the US, the Higher Education Act, 1965 had transferred all education responsibilities to the Department of Education. In the UK, both medical education and profession continue to be regulated by the General Medical Council (the MCI counterpart), which is different from the regulator for Higher Education. Composition of Councils In 2007-08, MCI, when fully constituted, was a 129 member body. The Ministry in its draft NCHRH Bill makes a case for reducing this size. The argument advanced is that such a large size makes the council unwieldy in character and hence constrains reform. In 2007-08, 71% of the members in the committee were elected. These represented universities and doctors registered across the country. However, the Standing Committee on H&FW report (2006) points out that delays in conducting elections usually leads to several vacancies in this category, thereby reducing the actual percentage of elected members. MCI’s 2007-08 annual report mentions that at the time of publishing the report, 29 seats (32% of elected category) were vacant due to ‘various reasons like expiry of term, non-election of a member, non-existence of medical faculty of certain Universities’. In November 2001, the Delhi High Court set aside the election of Dr. Ketan Desai as President of the MCI, stating that he had been elected under a ‘flawed constitution’. The central government had failed to ensure timely conduct of elections to the MCI. As a result, a number of seats were lying vacant. The Court ordered that the MCI be reconstituted at the earliest and appointed an administrator to oversee the functioning of the MCI until this was done. Several countries like the UK are amending their laws to make council membership more broad-based by including ‘lay-members’/ non-doctors. The General Medical Council in the UK was recently reconstituted and it now comprises of 24 members - 12 ‘lay’ and 12 medical members. (See http://www.gmc-uk.org/about/council.asp) Way ahead According to latest news reports, the MoH&FW is currently revising the draft Bill. Let's wait and see how the actual legislation shapes up. Watch this space for further updates!
As of April 22, 2020, Sikkim does not have any confirmed cases of COVID-19. As of April 21, 2020, 87 samples have been sent for testing from Sikkim. Of these, 80 have tested negative for COVID-19, and the results of seven samples are awaited. The state has announced several policy decisions to prevent the spread of the virus and provide relief for those affected by it. In this blog post, we summarise some of the key measures taken by the Sikkim state government in this regard as of April 22, 2020.
Response before national lockdown
On March 16, the state government responded to the growing number of suspected cases in India by notifying certain directions to be applicable till April 15, 2020. These included: (i) banning the entry of all domestic and foreign tourists in to the state, (ii) closing all educational institutes and anganwadis, (iii) prohibiting the use of recreational facilities such as, casinos, gym, and cinemas, (iii) closing three out of five check posts (border opening) for all visitors in to the state and opening the other two only for medical and police teams, and (iv) banning private industries from getting migrant workers from outside the state and avoiding large concentration of workers at one place.
On March 19, assembly of more than five people was prohibited in the state until April 15, 2020. The government ordered the suspension of all non-essential work on March 19. The supply of all essential commodities such as food grains, vegetables, sanitisers and masks was allowed. Further, the formation of a sub-divisional task force to detect suspected cases was ordered.
On March 22, the government regulated intra-state movement of private vehicles, two-wheelers and taxis on an odd-even basis (allowing plying of vehicles on alternate days as per the number plate) until April 15, 2020. The government also reduced the budget session of the state to two days on March 23.
On March 25, the central government announced on a 21-day country-wide lockdown till April 14. During the lockdown the state government took various steps for physical containment, health, financial and welfare measures. These are detailed below.
Measures taken during lockdown
Movement Restrictions
Certain movement restrictions were put across the state. These include:
Essential Goods and Services
On April 5, the state government issued an order requiring establishments such as shops, hotels, private offices, and commercial establishments to remain closed until April 15. Establishments which were permitted to remain functional include law enforcement agencies, health services, electricity and water services, petrol pumps, and media. Shops for PDS, groceries, vegetables, milk and, medicines were only allowed remain open from 9 am to 4 pm.
Health Measures
On March 31, the Sikkim government identified and set up dedicated isolation wards and treatment centres in the STNM hospital, Sochakgang as a precautionary measure. The government also issued directions for citizens to avoid getting infected by coronavirus. These included social distancing, and maintaining proper hygiene.
On April 18, the state government made it mandatory for all the public, students, teachers, and government employees, to install the Aarogya Setu application. The government of India launched a mobile app called ‘Aarogya Setu’ to enable people to assess the risk of catching COVID-19 on April 2, 2020. The app uses Bluetooth and Global Positioning System (GPS) based device location for contact tracing in order to prevent the spread of COVID-19.
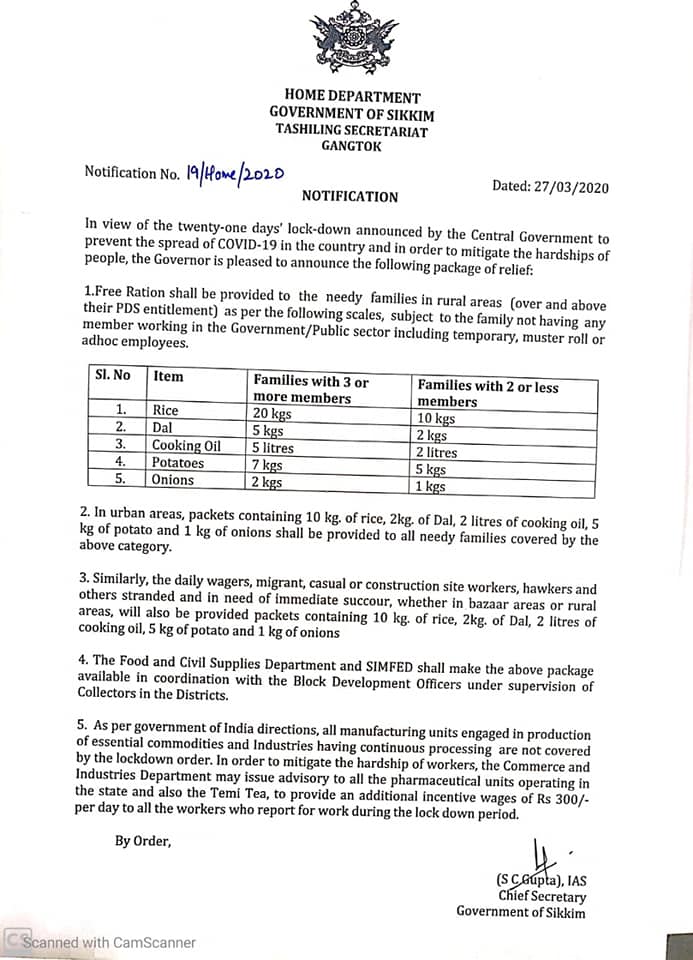
Welfare Measures
Certain relaxations after 20th April
On April 14, the nation-wide lockdown was further extended till May 3, 2020. On April 15, the Ministry of Home Affairs issued guidelines outlining select activities which will be permitted from April 20 onwards. These activities include health services, agriculture related activities, certain financial sector activities, operation of Anganwadis, MNREGA works, and cargo movement. Further, subject to certain conditions, commercial and private establishments, industrial establishments, government offices, and construction activities will also be permitted. The Sikkim government took the following steps in the same line.
For more information on the spread of COVID-19 and the central and state government response to the pandemic, please see here.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}