In the recent past, there has been a renewed discussion around nutrition in India. A few months ago, the Ministry of Health and Family Welfare had released the National Health Policy, 2017.[1] It highlighted the negative impact of malnutrition on the population’s productivity, and its contribution to mortality rates in the country. In light of the long term effects of malnutrition, across generations, the NITI Aayog released the National Nutrition Strategy this week. This post presents the current status of malnutrition in India and measures proposed by this Strategy.
What is malnutrition?
Malnutrition indicates that children are either too short for their age or too thin.[2] Children whose height is below the average for their age are considered to be stunted. Similarly, children whose weight is below the average for their age are considered thin for their height or wasted. Together, the stunted and wasted children are considered to be underweight – indicating a lack of proper nutritional intake and inadequate care post childbirth.
What is the extent of malnutrition in India?
India’s performance on key malnutrition indicators is poor according to national and international studies. According to UNICEF, India was at the 10th spot among countries with the highest number of underweight children, and at the 17th spot for the highest number of stunted children in the world.[3]
Malnutrition affects chances of survival for children, increases their susceptibility to illness, reduces their ability to learn, and makes them less productive in later life.[4] It is estimated that malnutrition is a contributing factor in about one-third of all deaths of children under the age of 5.[5] Figure 1 looks at the key statistics on malnutrition for children in India.
Figure 1: Malnutrition in children under 5 years (2005-06 and 2015-16)

Sources: National Family Health Survey 3 & 4; PRS.
Over the decade between 2005 and 2015, there has been an overall reduction in the proportion of underweight children in India, mainly on account of an improvement in stunting. While the percentage of stunted children under 5 reduced from 48% in 2005-06 to 38.4% in 2015-16, there has been a rise in the percentage of children who are wasted from 19.8% to 21% during this period.[6],[7] A high increase in the incidence of wasting was noted in Punjab, Goa, Maharashtra, Karnataka, and Sikkim.[8]
The prevalence of underweight children was found to be higher in rural areas (38%) than urban areas (29%). According to WHO, infants weighing less than 2.5 Kg are 20 times more likely to die than heavier babies.2 In India, the national average weight at birth is less than 2.5 Kg for 19% of the children. The incidence of low birth-weight babies varied across different states, with Madhya Pradesh, Rajasthan and Uttar Pradesh witnessing the highest number of underweight childbirths at 23%.[9]
Further, more than half of India’s children are anaemic (58%), indicating an inadequate amount of haemoglobin in the blood. This is caused by a nutritional deficiency of iron and other essential minerals, and vitamins in the body.2
Is malnutrition witnessed only among children?
No. Among adults, 23% of women and 20% of men are considered undernourished in India. On the other hand, 21% of women and 19% of men are overweight or obese. The simultaneous occurrence of over nutrition and under-nutrition indicates that adults in India are suffering from a dual burden of malnutrition (abnormal thinness and obesity). This implies that about 56% of women and 61% of men are at normal weight for their height.
What does the National Nutrition Strategy propose?
Various government initiatives have been launched over the years which seek to improve the nutrition status in the country. These include the Integrated Child Development Services (ICDS), the National Health Mission, the Janani Suraksha Yojana, the Matritva Sahyog Yojana, the Mid-Day Meal Scheme, and the National Food Security Mission, among others. However, concerns regarding malnutrition have persisted despite improvements over the years. It is in this context that the National Nutrition Strategy has been released. Key features of the Strategy include:8
[1] National Health Policy, 2017, Ministry of Health and Family Welfare, March 16, 2017, http://mohfw.nic.in/showfile.php?lid=4275
[2] Nutrition in India, Ministry of Health and Family Welfare, 2005-06, http://rchiips.org/nfhs/nutrition_report_for_website_18sep09.pdf
[3] Unstarred Question No. 2759, Lok Sabha, Answered on March 17, 2017, http://164.100.47.190/loksabhaquestions/annex/11/AU2759.pdf
[4] Helping India Combat Persistently High Rates of Malnutrition, The World Bank, May 13, 2013, http://www.worldbank.org/en/news/feature/2013/05/13/helping-india-combat-persistently-high-rates-of-malnutrition
[5] Unstarred Question No. 4902, Lok Sabha, Answered on December 16, 2016, http://164.100.47.190/loksabhaquestions/annex/10/AU4902.pdf
[6] National Family Health Survey – 3, 2005-6, Ministry of Health and Family Welfare http://rchiips.org/nfhs/pdf/India.pdf
[7] National Family Health Survey – 4 , 2015-16, Ministry of Health and Family Welfare, http://rchiips.org/NFHS/pdf/NFHS4/India.pdf
[8] National Nutrition Strategy, 2017, NITI Aayog, September 2017, http://niti.gov.in/writereaddata/files/document_publication/Nutrition_Strategy_Booklet.pdf
[9] Rapid Survey On Children, Ministry of Women and Child Development, 2013-14, http://wcd.nic.in/sites/default/files/RSOC%20National%20Report%202013-14%20Final.pdf
As of May 11, 2020, there are 67,152 confirmed cases of COVID-19 in India. Since May 4, 24,619 new cases have been registered. Out of the confirmed cases so far, 20,917 patients have been cured/discharged and 2,206 have died. As the spread of COVID-19 has increased across the country, the central government has continued to announce several policy decisions to contain the spread, and support citizens and businesses who are being affected by the pandemic. In this blog post, we summarise some of the key measures taken by the central government in this regard between May 4 and May 11, 2020.
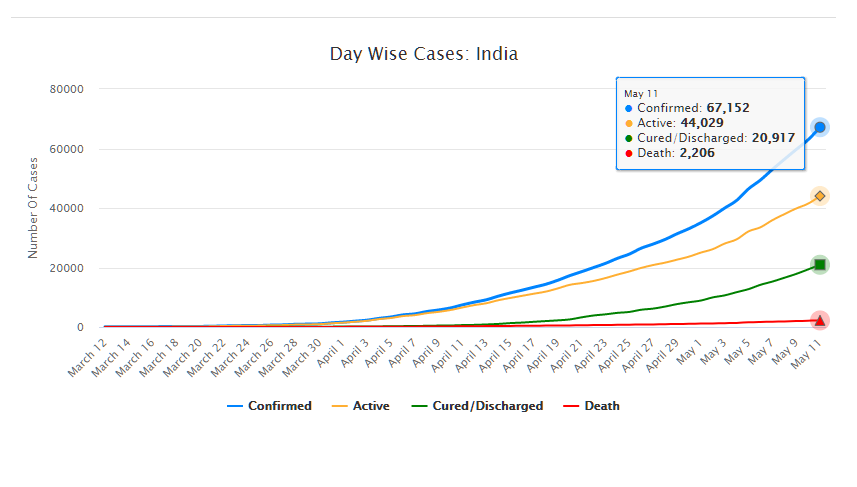
Source: Ministry of Health and Family Welfare; PRS.
Industry
Relaxation of labour laws in some states
The Gujarat, Himachal Pradesh, Rajasthan, Haryana, and Uttarakhand governments have passed notifications to increase maximum weekly work hours from 48 hours to 72 hours and daily work hours from 9 hours to 12 hours for certain factories. This was done to combat the shortage of labour caused by the lockdown. Further, some state governments stated that longer shifts would ensure a fewer number of workers in factories so as to allow for social distancing.
Madhya Pradesh has promulgated the Madhya Pradesh Labour Laws (Amendment) Ordinance, 2020. The Ordinance exempts establishments with less than 100 workers from adhering to the Madhya Pradesh Industrial Employment (Standing Orders) Act, 1961, which regulates the conditions of employment of workers. Further, it allows the state government to exempt any establishment or class of establishments from the Madhya Pradesh Shram Kalyan Nidhi Adhiniyam, 1982, which provides for the constitution of a welfare fund for labour.
The Uttar Pradesh government has published a draft Ordinance which exempts all factories and establishments engaged in manufacturing processes from all labour laws for a period of three years. Certain conditions will continue to apply with regard to payment of wages, safety, compensation and work hours, amongst others. However, labour laws providing for social security, industrial dispute resolution, trade unions, strikes, amongst others, will not apply under the Ordinance.
Financial aid
Central government signs an agreement with Asian Infrastructure Investment Bank for COVID-19 support
The central government and Asian Infrastructure Investment Bank (AIIB) signed a 500 million dollar agreement for the COVID-19 Emergency Response and Health Systems Preparedness Project. The project aims to help India respond to the COVID-19 pandemic and strengthen India’s public health system to manage future disease outbreaks. The project is being financed by the World Bank and AIIB in the amount of 1.5 billion dollars, of which one billion dollars is being provided by World Bank and 500 million dollars is being provided by AIIB. This financial support will be available to all states and union territories and will be used to address the needs of at-risk populations, medical personnel, and creating medical and testing facilities, amongst others. The project will be implemented by the National Health Mission, the National Center for Disease Control, and the Indian Council of Medical Research, under the Ministry of Health and Family Welfare.
Travel
Restarting of passenger travel by railways
Indian Railways plans to restart passenger trains from May 12 onwards. It will begin with 15 pairs of trains which will run from New Delhi station connecting Dibrugarh, Agartala, Howrah, Patna, Bilaspur, Ranchi, Bhubaneswar, Secunderabad, Bengaluru, Chennai, Thiruvananthapuram, Madgaon, Mumbai Central, Ahmedabad and Jammu Tawi. Booking for reservation in these trains will start at 4 pm on May 11. Thereafter, Indian Railways plans to start more services on new routes.
Return of Indians stranded abroad
The central government will facilitate the return of Indian nationals stranded abroad in a phased manner beginning on May 7. The travel will be arranged by aircraft and naval ships. The stranded Indians utilising the service will be required to pay for it. Medical screening of the passengers will be done before the flight. On reaching India, passengers will be required to download the Aarogya Setu app. Further, they will be quarantined by the concerned state government in either a hospital or a quarantine institution for 14 days on a payment basis. After quarantine, passengers will be tested for COVID-19 and further action will be taken based on the results.
For more information on the spread of COVID-19 and the central and state government response to the pandemic, please see here.

