This post is pursuant to the discussion on population stabilization being held in Parliament currently. India is the second most populous country in the world, sustaining 16.7% of the world's population on 2.4% of the world's surface area. The population of the country has increased from 238 million in 1901 to 1,029 million in 2001. Even now, India continues to add about 26 million people per year. This is because more than 50% of the population is in the reproductive age group. India launched a family planning programme in 1952. Though the birth rate started decreasing, it was accompanied by a sharp decrease in death rate, leading to an overall increase in population. In 1976, the first National Population Policy was formulated and tabled in Parliament. However, the statement was neither discussed nor adopted. The National Health Policy was then designed in 1983. It stressed the need for ‘securing the small family norm, through voluntary efforts and moving towards the goal of population stabilization’. While adopting the Health Policy, Parliament emphasized the need for a separate National Population Policy. This was followed by the National Population Policy in 2000. The immediate objective of the policy was to address the unmet needs for contraception, health care infrastructure and personnel, and to provide integrated service delivery for basic reproductive and child health care. The medium-term objective was to bring TFR (Total Fertility Rate - the average number of children a woman bears over her lifetime) to replacement levels by 2010. In the long term, it targeted a stable population by 2045, ‘at a level consistent with the requirements of sustainable economic growth, social development, and environmental protection.’ (See http://populationcommission.nic.in/npp.htm) Total Fertility Rate India’s TFR was around 6.1 in 1961. This meant that an average woman bore over 6 children during her lifetime. Over the years, there has been a noticeable decrease in this figure. The latest National Family Health Survey (NFHS III, 2005-06) puts it at 2.7. TFR is almost one child higher in rural areas (3.0) than in urban areas (2.1). TFR also varies widely across states. The states of Andhra Pradesh, Goa, Himachal Pradesh, Karnataka, Kerala, Maharashtra, Punjab, Sikkim and Tamil Nadu have reached a TFR of 2.1 or less. However, several other states like UP, Bihar, MP, Rajasthan, Orissa, Uttaranchal, Jharkhand and Chhattisgarh, where over 40% of the population lives, TFR is still high. (See http://www.jsk.gov.in/total_fertility_rate.asp) Factors that affect population growth The overarching factor that affects population growth is low socio-economic development. For example, Uttar Pradesh has a literacy rate of 56%; only 14% of the women receive complete antenatal care. Uttar Pradesh records an average of four children per couple. In contrast, in Kerala almost every person is literate and almost every woman receives antenatal care. Kerala records an average of two children per couple. Infant mortality In 1961, the Infant Mortality Rate (IMR), deaths of infants per 1000 live births, was 115. The current all India average is much lower at 57. However, in most developed countries this figure is less than 5. IMR is the lowest at 15 in Kerala and the highest at 73 in Uttar Pradesh. Empirical correlations suggest that high IMR leads to greater desire for children. Early marriage Nationwide almost 43% of married women aged 20-24 were married before the age of 18. This figure is as high as 68% in Bihar. Not only does early marriage increase the likelihood of more children, it also puts the woman's health at risk. Level of education Fertility usually declines with increase in education levels of women. Use of contraceptives According to NFHS III (2005-06), only 56% of currently married women use some method of family planning in India. A majority of them (37%) have adopted permanent methods like sterilization. Other socio-economic factors The desire for larger families particularly preference for a male child also leads to higher birth rates. It is estimated that preference for a male child and high infant mortality together account for 20% of the total births in the country. Government initiatives The National Population Policy 2000 gave a focused approach to the problem of population stabilization. Following the policy, the government also enacted the Constitution (84th Amendment) Act, 2002. This Amendment extended the freeze on the state-wise allocation of seats in the Lok Sabha and the Rajya Sabha to 2026. It was expected that this would serve ‘as a motivational measure, in order to enable state governments to fearlessly and effectively pursue the agenda for population stabilization contained in the National Population Policy, 2000’. The National Commission on Population was formed in the year 2000. The Commission, chaired by the Prime Minister, has the mandate to review, monitor and give directions for implementation of the National Population Policy. The Jansankhya Sthirata Kosh (National Population Stabilization Fund) was setup as an autonomous society of the Ministry of Health and Family Welfare in 2005. Its broad mandate is to undertake activities aimed at achieving population stabilization. Programmes like the National Rural Health Mission, Janani Suraksha Yojana, ICDS (Integrated Child Development Services) etc. have also been launched by the government to tackle the healthcare needs of people. This is also expected to contribute to population stabilization. Free contraceptives are also being provided. In addition, monetary incentives are given to couples undertaking permanent family planning methods like vasectomy and tubectomy. Nutritional and educational problems are being targeted through programs like the mid-day meal scheme and the recently enacted Right to Education. ---------------- For more details on the issue, see the website of the National Population Stabilization Fund (http://www.jsk.gov.in/) Sources: Registrar General, India National Population Stabilization Fund National Commission on Population National Family Health Survey III (2005-06)
As of May 11, 2020, there are 67,152 confirmed cases of COVID-19 in India. Since May 4, 24,619 new cases have been registered. Out of the confirmed cases so far, 20,917 patients have been cured/discharged and 2,206 have died. As the spread of COVID-19 has increased across the country, the central government has continued to announce several policy decisions to contain the spread, and support citizens and businesses who are being affected by the pandemic. In this blog post, we summarise some of the key measures taken by the central government in this regard between May 4 and May 11, 2020.
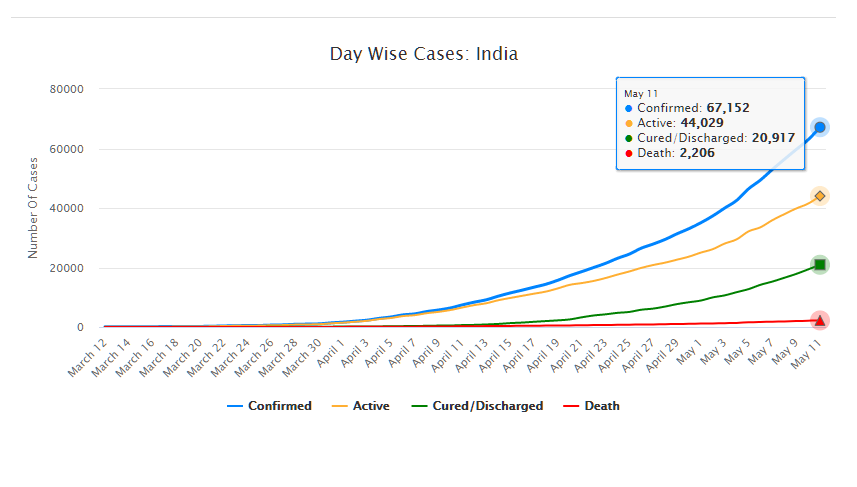
Source: Ministry of Health and Family Welfare; PRS.
Industry
Relaxation of labour laws in some states
The Gujarat, Himachal Pradesh, Rajasthan, Haryana, and Uttarakhand governments have passed notifications to increase maximum weekly work hours from 48 hours to 72 hours and daily work hours from 9 hours to 12 hours for certain factories. This was done to combat the shortage of labour caused by the lockdown. Further, some state governments stated that longer shifts would ensure a fewer number of workers in factories so as to allow for social distancing.
Madhya Pradesh has promulgated the Madhya Pradesh Labour Laws (Amendment) Ordinance, 2020. The Ordinance exempts establishments with less than 100 workers from adhering to the Madhya Pradesh Industrial Employment (Standing Orders) Act, 1961, which regulates the conditions of employment of workers. Further, it allows the state government to exempt any establishment or class of establishments from the Madhya Pradesh Shram Kalyan Nidhi Adhiniyam, 1982, which provides for the constitution of a welfare fund for labour.
The Uttar Pradesh government has published a draft Ordinance which exempts all factories and establishments engaged in manufacturing processes from all labour laws for a period of three years. Certain conditions will continue to apply with regard to payment of wages, safety, compensation and work hours, amongst others. However, labour laws providing for social security, industrial dispute resolution, trade unions, strikes, amongst others, will not apply under the Ordinance.
Financial aid
Central government signs an agreement with Asian Infrastructure Investment Bank for COVID-19 support
The central government and Asian Infrastructure Investment Bank (AIIB) signed a 500 million dollar agreement for the COVID-19 Emergency Response and Health Systems Preparedness Project. The project aims to help India respond to the COVID-19 pandemic and strengthen India’s public health system to manage future disease outbreaks. The project is being financed by the World Bank and AIIB in the amount of 1.5 billion dollars, of which one billion dollars is being provided by World Bank and 500 million dollars is being provided by AIIB. This financial support will be available to all states and union territories and will be used to address the needs of at-risk populations, medical personnel, and creating medical and testing facilities, amongst others. The project will be implemented by the National Health Mission, the National Center for Disease Control, and the Indian Council of Medical Research, under the Ministry of Health and Family Welfare.
Travel
Restarting of passenger travel by railways
Indian Railways plans to restart passenger trains from May 12 onwards. It will begin with 15 pairs of trains which will run from New Delhi station connecting Dibrugarh, Agartala, Howrah, Patna, Bilaspur, Ranchi, Bhubaneswar, Secunderabad, Bengaluru, Chennai, Thiruvananthapuram, Madgaon, Mumbai Central, Ahmedabad and Jammu Tawi. Booking for reservation in these trains will start at 4 pm on May 11. Thereafter, Indian Railways plans to start more services on new routes.
Return of Indians stranded abroad
The central government will facilitate the return of Indian nationals stranded abroad in a phased manner beginning on May 7. The travel will be arranged by aircraft and naval ships. The stranded Indians utilising the service will be required to pay for it. Medical screening of the passengers will be done before the flight. On reaching India, passengers will be required to download the Aarogya Setu app. Further, they will be quarantined by the concerned state government in either a hospital or a quarantine institution for 14 days on a payment basis. After quarantine, passengers will be tested for COVID-19 and further action will be taken based on the results.
For more information on the spread of COVID-19 and the central and state government response to the pandemic, please see here.

