As of April 22, 2020, Sikkim does not have any confirmed cases of COVID-19. As of April 21, 2020, 87 samples have been sent for testing from Sikkim. Of these, 80 have tested negative for COVID-19, and the results of seven samples are awaited. The state has announced several policy decisions to prevent the spread of the virus and provide relief for those affected by it. In this blog post, we summarise some of the key measures taken by the Sikkim state government in this regard as of April 22, 2020.
Response before national lockdown
On March 16, the state government responded to the growing number of suspected cases in India by notifying certain directions to be applicable till April 15, 2020. These included: (i) banning the entry of all domestic and foreign tourists in to the state, (ii) closing all educational institutes and anganwadis, (iii) prohibiting the use of recreational facilities such as, casinos, gym, and cinemas, (iii) closing three out of five check posts (border opening) for all visitors in to the state and opening the other two only for medical and police teams, and (iv) banning private industries from getting migrant workers from outside the state and avoiding large concentration of workers at one place.
On March 19, assembly of more than five people was prohibited in the state until April 15, 2020. The government ordered the suspension of all non-essential work on March 19. The supply of all essential commodities such as food grains, vegetables, sanitisers and masks was allowed. Further, the formation of a sub-divisional task force to detect suspected cases was ordered.
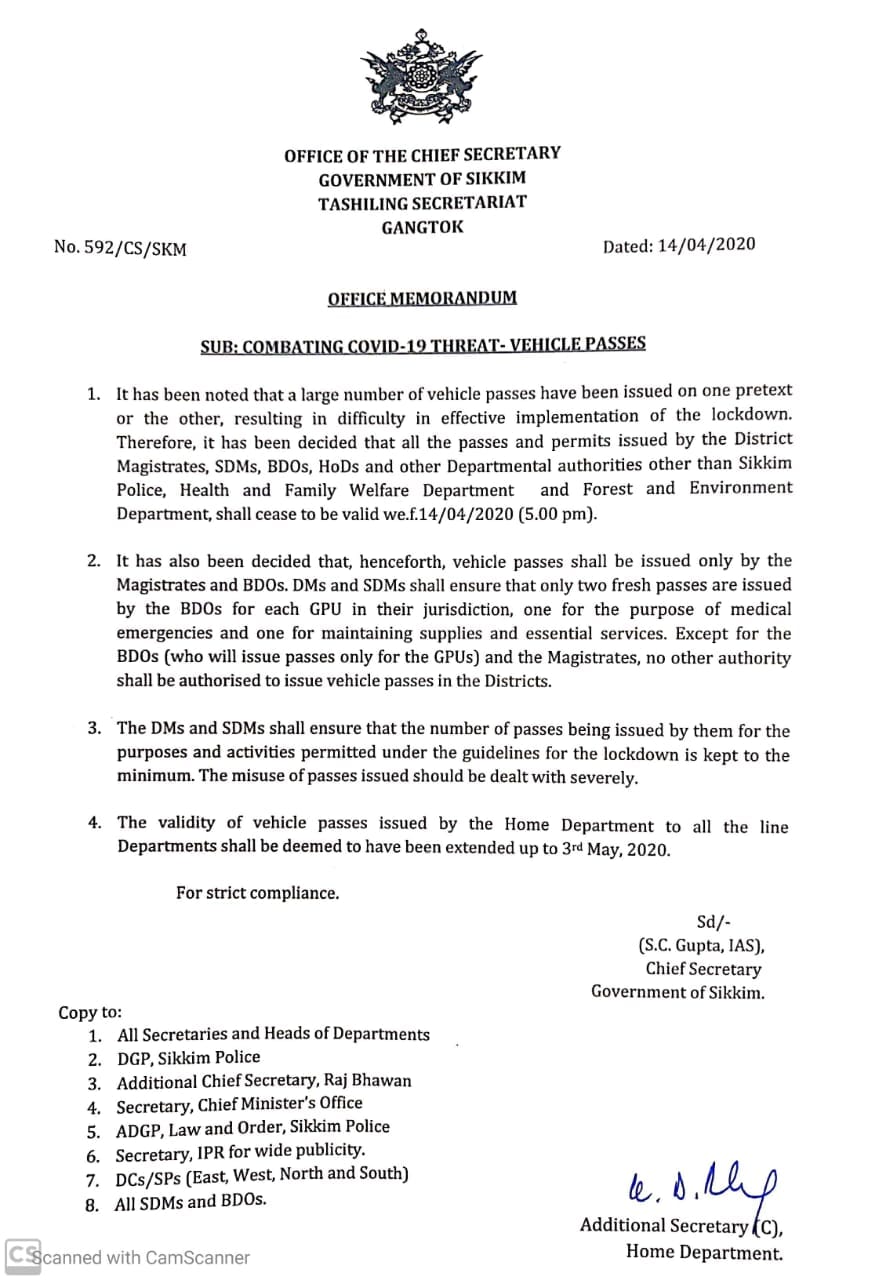
On March 22, the government regulated intra-state movement of private vehicles, two-wheelers and taxis on an odd-even basis (allowing plying of vehicles on alternate days as per the number plate) until April 15, 2020. The government also reduced the budget session of the state to two days on March 23.
On March 25, the central government announced on a 21-day country-wide lockdown till April 14. During the lockdown the state government took various steps for physical containment, health, financial and welfare measures. These are detailed below.
Measures taken during lockdown
Movement Restrictions
Certain movement restrictions were put across the state. These include:
Essential Goods and Services
On April 5, the state government issued an order requiring establishments such as shops, hotels, private offices, and commercial establishments to remain closed until April 15. Establishments which were permitted to remain functional include law enforcement agencies, health services, electricity and water services, petrol pumps, and media. Shops for PDS, groceries, vegetables, milk and, medicines were only allowed remain open from 9 am to 4 pm.
Health Measures
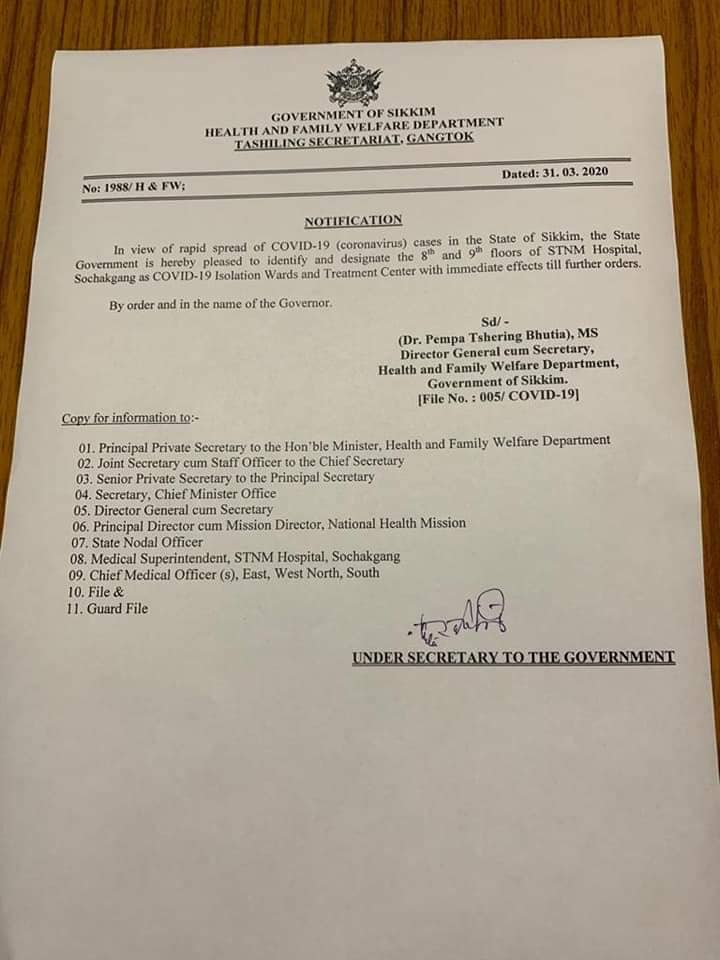
On March 31, the Sikkim government identified and set up dedicated isolation wards and treatment centres in the STNM hospital, Sochakgang as a precautionary measure. The government also issued directions for citizens to avoid getting infected by coronavirus. These included social distancing, and maintaining proper hygiene.
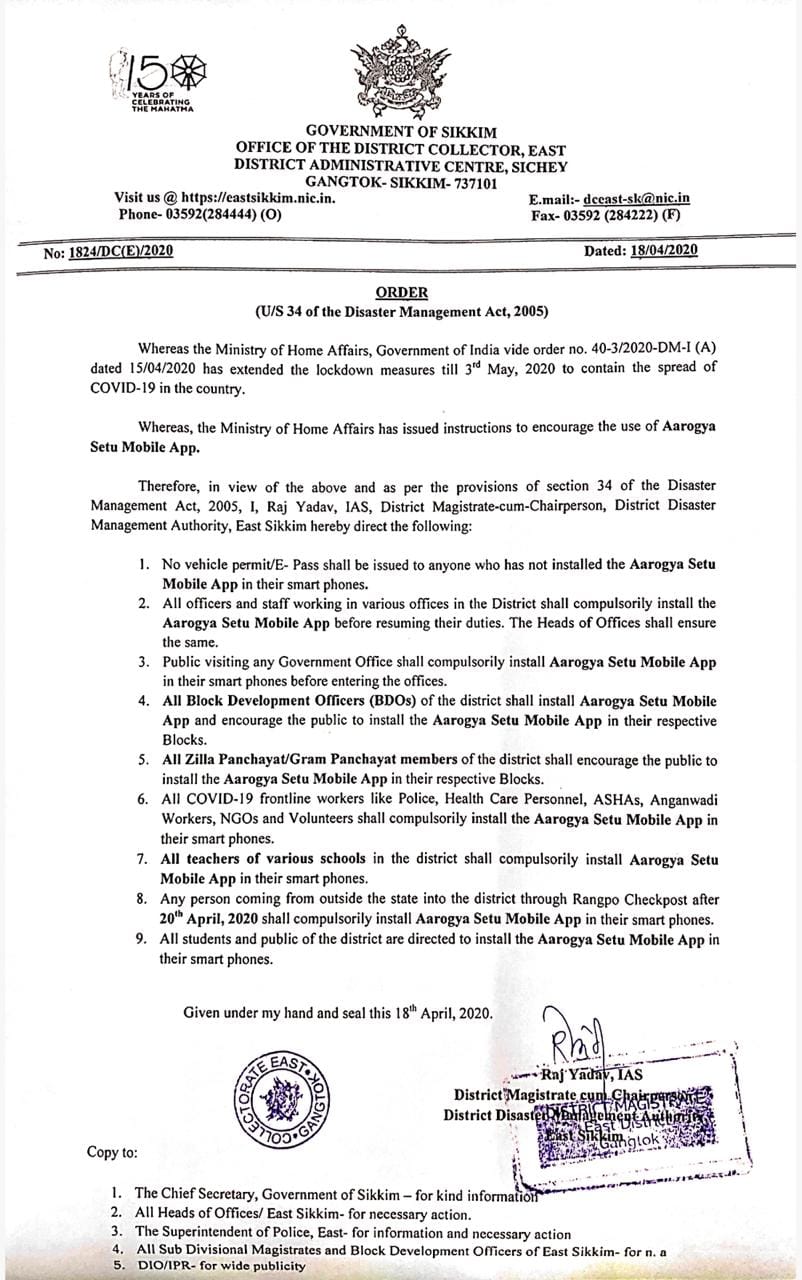
On April 18, the state government made it mandatory for all the public, students, teachers, and government employees, to install the Aarogya Setu application. The government of India launched a mobile app called ‘Aarogya Setu’ to enable people to assess the risk of catching COVID-19 on April 2, 2020. The app uses Bluetooth and Global Positioning System (GPS) based device location for contact tracing in order to prevent the spread of COVID-19.
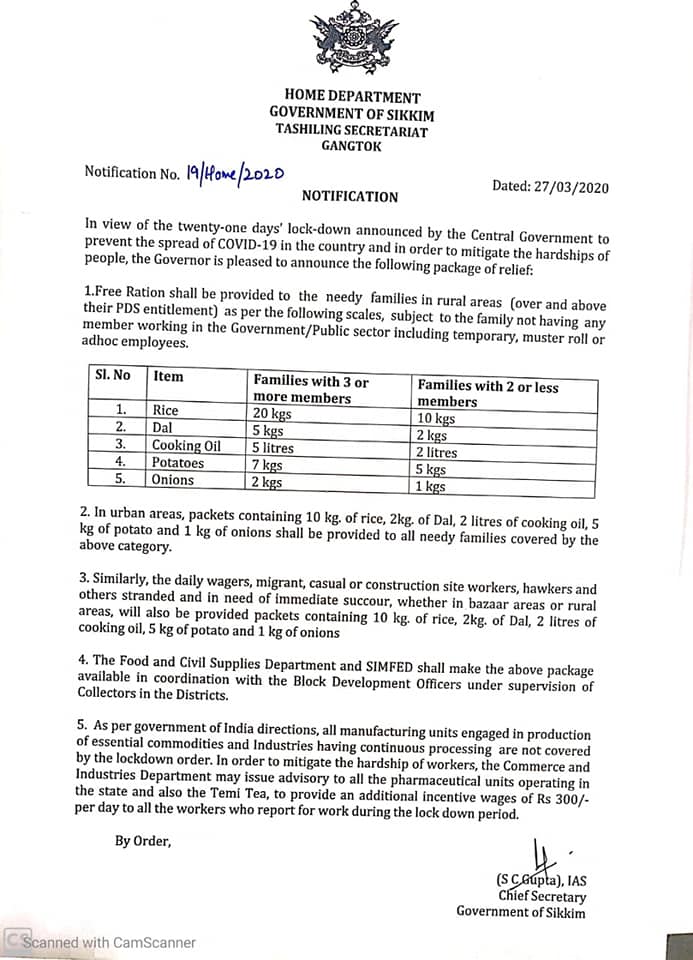
Welfare Measures
Certain relaxations after 20th April
On April 14, the nation-wide lockdown was further extended till May 3, 2020. On April 15, the Ministry of Home Affairs issued guidelines outlining select activities which will be permitted from April 20 onwards. These activities include health services, agriculture related activities, certain financial sector activities, operation of Anganwadis, MNREGA works, and cargo movement. Further, subject to certain conditions, commercial and private establishments, industrial establishments, government offices, and construction activities will also be permitted. The Sikkim government took the following steps in the same line.
For more information on the spread of COVID-19 and the central and state government response to the pandemic, please see here.
In the recent past, there has been a renewed discussion around nutrition in India. A few months ago, the Ministry of Health and Family Welfare had released the National Health Policy, 2017.[1] It highlighted the negative impact of malnutrition on the population’s productivity, and its contribution to mortality rates in the country. In light of the long term effects of malnutrition, across generations, the NITI Aayog released the National Nutrition Strategy this week. This post presents the current status of malnutrition in India and measures proposed by this Strategy.
What is malnutrition?
Malnutrition indicates that children are either too short for their age or too thin.[2] Children whose height is below the average for their age are considered to be stunted. Similarly, children whose weight is below the average for their age are considered thin for their height or wasted. Together, the stunted and wasted children are considered to be underweight – indicating a lack of proper nutritional intake and inadequate care post childbirth.
What is the extent of malnutrition in India?
India’s performance on key malnutrition indicators is poor according to national and international studies. According to UNICEF, India was at the 10th spot among countries with the highest number of underweight children, and at the 17th spot for the highest number of stunted children in the world.[3]
Malnutrition affects chances of survival for children, increases their susceptibility to illness, reduces their ability to learn, and makes them less productive in later life.[4] It is estimated that malnutrition is a contributing factor in about one-third of all deaths of children under the age of 5.[5] Figure 1 looks at the key statistics on malnutrition for children in India.
Figure 1: Malnutrition in children under 5 years (2005-06 and 2015-16)

Sources: National Family Health Survey 3 & 4; PRS.
Over the decade between 2005 and 2015, there has been an overall reduction in the proportion of underweight children in India, mainly on account of an improvement in stunting. While the percentage of stunted children under 5 reduced from 48% in 2005-06 to 38.4% in 2015-16, there has been a rise in the percentage of children who are wasted from 19.8% to 21% during this period.[6],[7] A high increase in the incidence of wasting was noted in Punjab, Goa, Maharashtra, Karnataka, and Sikkim.[8]
The prevalence of underweight children was found to be higher in rural areas (38%) than urban areas (29%). According to WHO, infants weighing less than 2.5 Kg are 20 times more likely to die than heavier babies.2 In India, the national average weight at birth is less than 2.5 Kg for 19% of the children. The incidence of low birth-weight babies varied across different states, with Madhya Pradesh, Rajasthan and Uttar Pradesh witnessing the highest number of underweight childbirths at 23%.[9]
Further, more than half of India’s children are anaemic (58%), indicating an inadequate amount of haemoglobin in the blood. This is caused by a nutritional deficiency of iron and other essential minerals, and vitamins in the body.2
Is malnutrition witnessed only among children?
No. Among adults, 23% of women and 20% of men are considered undernourished in India. On the other hand, 21% of women and 19% of men are overweight or obese. The simultaneous occurrence of over nutrition and under-nutrition indicates that adults in India are suffering from a dual burden of malnutrition (abnormal thinness and obesity). This implies that about 56% of women and 61% of men are at normal weight for their height.
What does the National Nutrition Strategy propose?
Various government initiatives have been launched over the years which seek to improve the nutrition status in the country. These include the Integrated Child Development Services (ICDS), the National Health Mission, the Janani Suraksha Yojana, the Matritva Sahyog Yojana, the Mid-Day Meal Scheme, and the National Food Security Mission, among others. However, concerns regarding malnutrition have persisted despite improvements over the years. It is in this context that the National Nutrition Strategy has been released. Key features of the Strategy include:8
[1] National Health Policy, 2017, Ministry of Health and Family Welfare, March 16, 2017, http://mohfw.nic.in/showfile.php?lid=4275
[2] Nutrition in India, Ministry of Health and Family Welfare, 2005-06, http://rchiips.org/nfhs/nutrition_report_for_website_18sep09.pdf
[3] Unstarred Question No. 2759, Lok Sabha, Answered on March 17, 2017, http://164.100.47.190/loksabhaquestions/annex/11/AU2759.pdf
[4] Helping India Combat Persistently High Rates of Malnutrition, The World Bank, May 13, 2013, http://www.worldbank.org/en/news/feature/2013/05/13/helping-india-combat-persistently-high-rates-of-malnutrition
[5] Unstarred Question No. 4902, Lok Sabha, Answered on December 16, 2016, http://164.100.47.190/loksabhaquestions/annex/10/AU4902.pdf
[6] National Family Health Survey – 3, 2005-6, Ministry of Health and Family Welfare http://rchiips.org/nfhs/pdf/India.pdf
[7] National Family Health Survey – 4 , 2015-16, Ministry of Health and Family Welfare, http://rchiips.org/NFHS/pdf/NFHS4/India.pdf
[8] National Nutrition Strategy, 2017, NITI Aayog, September 2017, http://niti.gov.in/writereaddata/files/document_publication/Nutrition_Strategy_Booklet.pdf
[9] Rapid Survey On Children, Ministry of Women and Child Development, 2013-14, http://wcd.nic.in/sites/default/files/RSOC%20National%20Report%202013-14%20Final.pdf


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}