As of April 22, 2020, Sikkim does not have any confirmed cases of COVID-19. As of April 21, 2020, 87 samples have been sent for testing from Sikkim. Of these, 80 have tested negative for COVID-19, and the results of seven samples are awaited. The state has announced several policy decisions to prevent the spread of the virus and provide relief for those affected by it. In this blog post, we summarise some of the key measures taken by the Sikkim state government in this regard as of April 22, 2020.
Response before national lockdown
On March 16, the state government responded to the growing number of suspected cases in India by notifying certain directions to be applicable till April 15, 2020. These included: (i) banning the entry of all domestic and foreign tourists in to the state, (ii) closing all educational institutes and anganwadis, (iii) prohibiting the use of recreational facilities such as, casinos, gym, and cinemas, (iii) closing three out of five check posts (border opening) for all visitors in to the state and opening the other two only for medical and police teams, and (iv) banning private industries from getting migrant workers from outside the state and avoiding large concentration of workers at one place.
On March 19, assembly of more than five people was prohibited in the state until April 15, 2020. The government ordered the suspension of all non-essential work on March 19. The supply of all essential commodities such as food grains, vegetables, sanitisers and masks was allowed. Further, the formation of a sub-divisional task force to detect suspected cases was ordered.
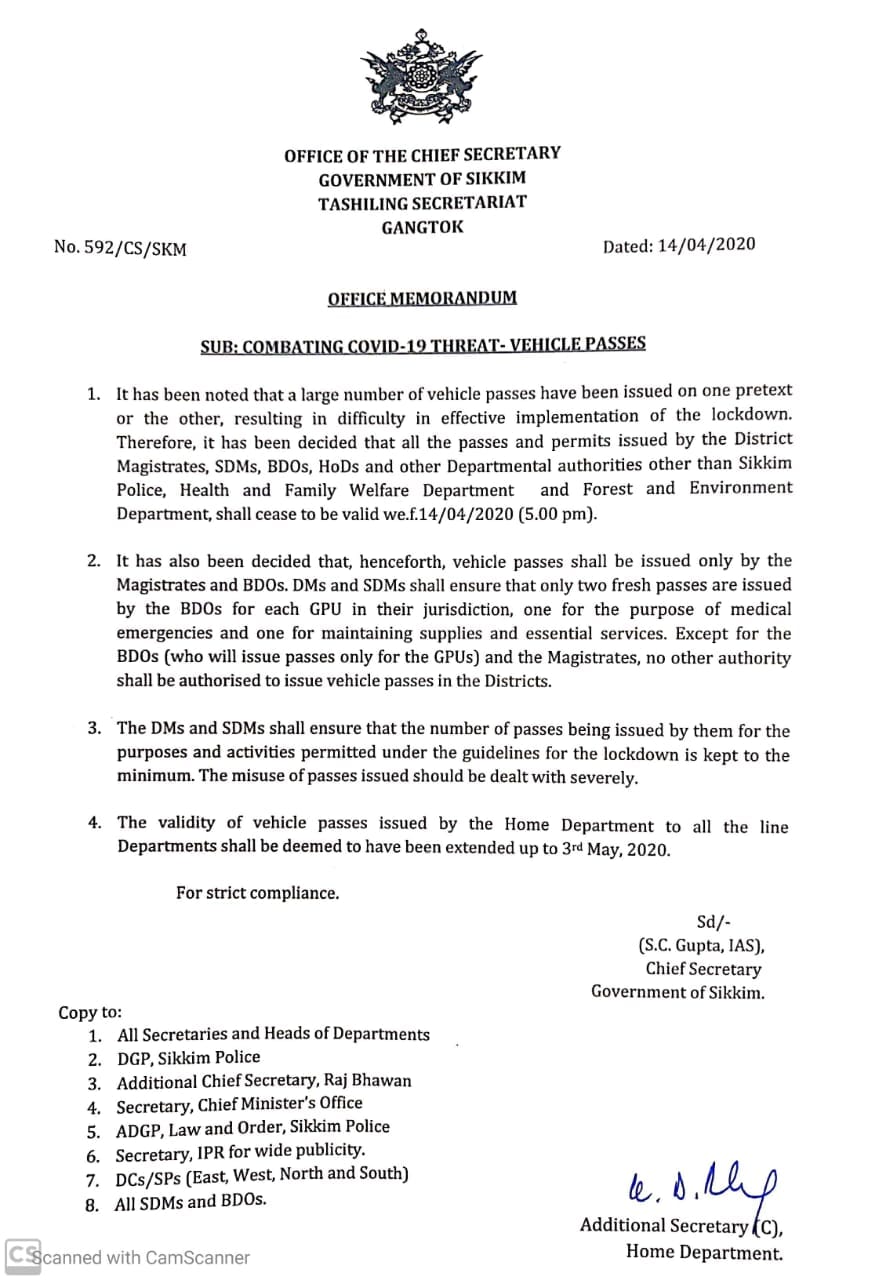
On March 22, the government regulated intra-state movement of private vehicles, two-wheelers and taxis on an odd-even basis (allowing plying of vehicles on alternate days as per the number plate) until April 15, 2020. The government also reduced the budget session of the state to two days on March 23.
On March 25, the central government announced on a 21-day country-wide lockdown till April 14. During the lockdown the state government took various steps for physical containment, health, financial and welfare measures. These are detailed below.
Measures taken during lockdown
Movement Restrictions
Certain movement restrictions were put across the state. These include:
Essential Goods and Services
On April 5, the state government issued an order requiring establishments such as shops, hotels, private offices, and commercial establishments to remain closed until April 15. Establishments which were permitted to remain functional include law enforcement agencies, health services, electricity and water services, petrol pumps, and media. Shops for PDS, groceries, vegetables, milk and, medicines were only allowed remain open from 9 am to 4 pm.
Health Measures
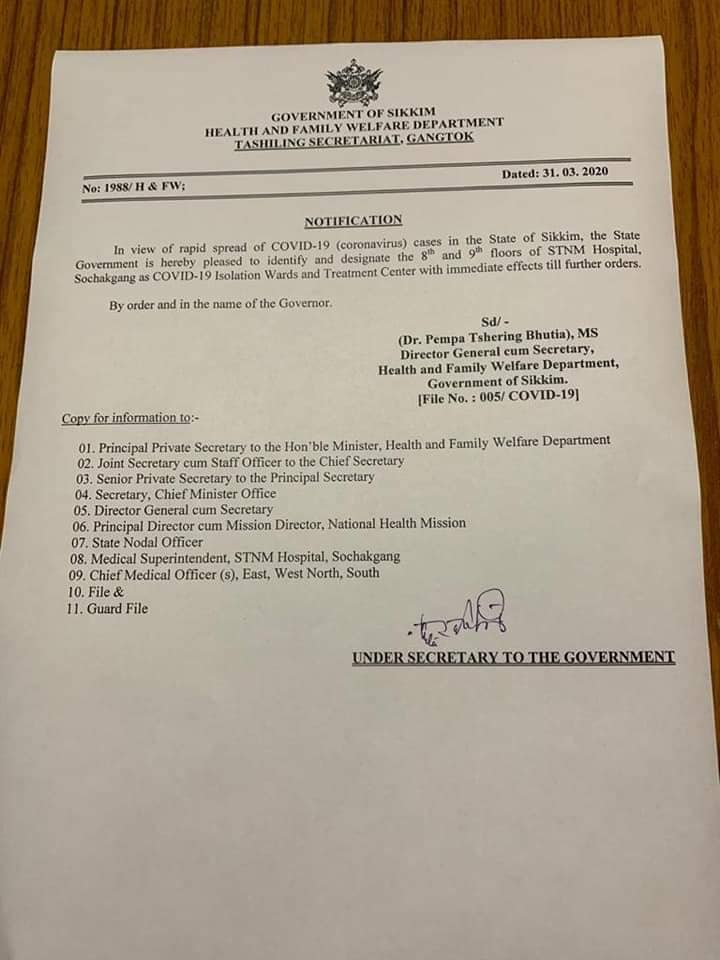
On March 31, the Sikkim government identified and set up dedicated isolation wards and treatment centres in the STNM hospital, Sochakgang as a precautionary measure. The government also issued directions for citizens to avoid getting infected by coronavirus. These included social distancing, and maintaining proper hygiene.
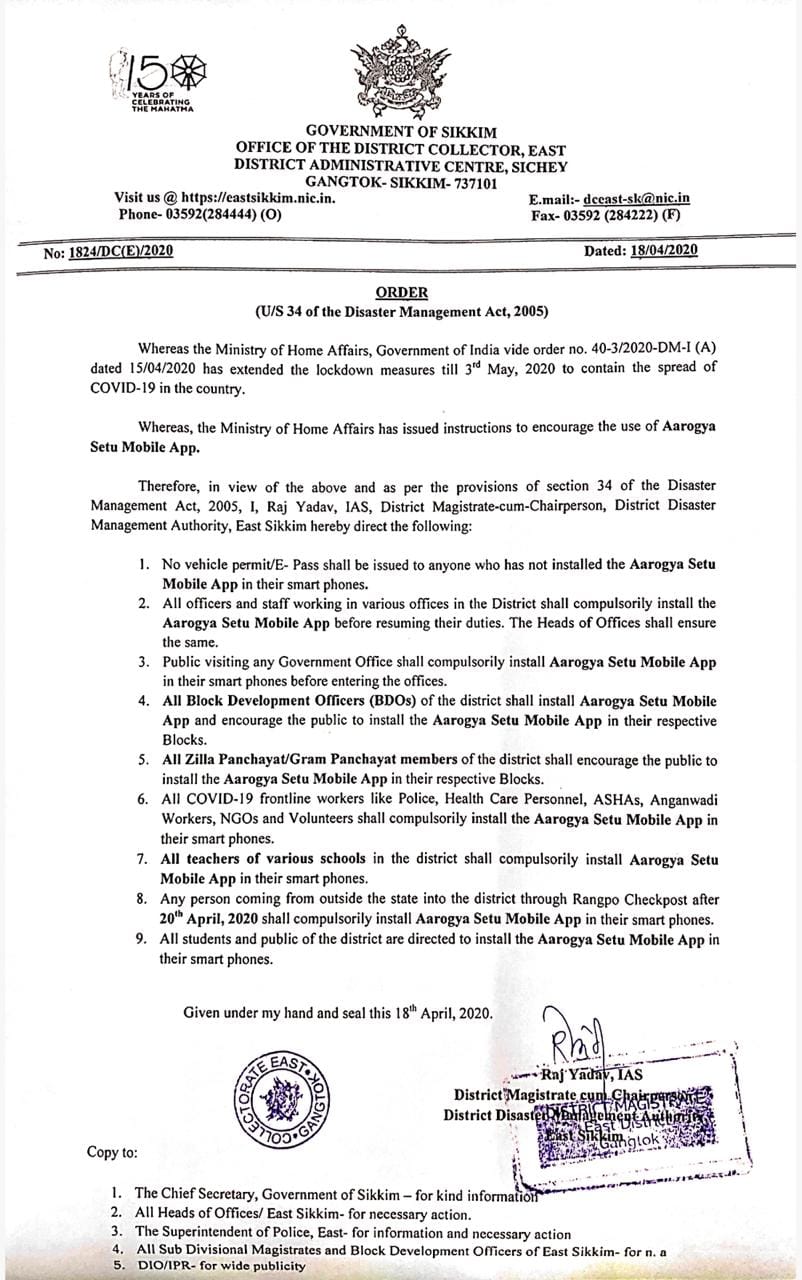
On April 18, the state government made it mandatory for all the public, students, teachers, and government employees, to install the Aarogya Setu application. The government of India launched a mobile app called ‘Aarogya Setu’ to enable people to assess the risk of catching COVID-19 on April 2, 2020. The app uses Bluetooth and Global Positioning System (GPS) based device location for contact tracing in order to prevent the spread of COVID-19.
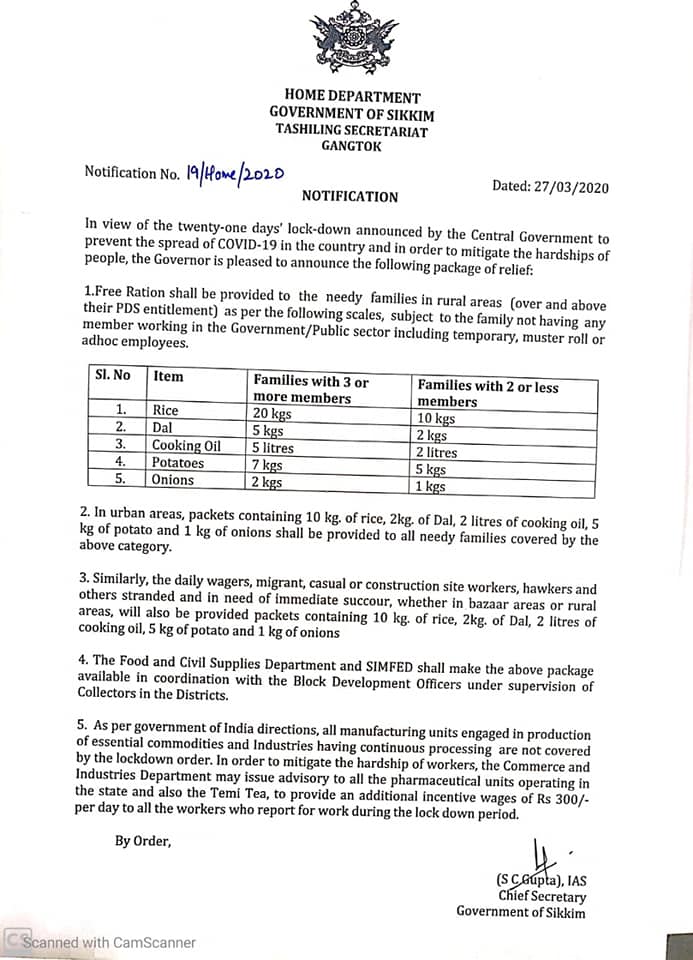
Welfare Measures
Certain relaxations after 20th April
On April 14, the nation-wide lockdown was further extended till May 3, 2020. On April 15, the Ministry of Home Affairs issued guidelines outlining select activities which will be permitted from April 20 onwards. These activities include health services, agriculture related activities, certain financial sector activities, operation of Anganwadis, MNREGA works, and cargo movement. Further, subject to certain conditions, commercial and private establishments, industrial establishments, government offices, and construction activities will also be permitted. The Sikkim government took the following steps in the same line.
For more information on the spread of COVID-19 and the central and state government response to the pandemic, please see here.
Recently, the Standing Committee on Health and Family Welfare submitted its report to the Parliament on the National Commission for Human Resource for Health Bill, 2011. The objective of the Bill is to “ensure adequate availability of human resources in the health sector in all states”. It seeks to set up the National Commission for Human Resources for Health (NCHRH), National Board for Health Education (NBHE), and the National Evaluation and Assessment Council (NEAC) in order to determine and regulate standards of health education in the country. It separates regulation of the education sector from that of professions such as law, medicine and nursing, and establishes professional councils at the national and state levels to regulate the professions. See here for PRS Bill Summary. The Standing Committee recommended that this Bill be withdrawn and a revised Bill be introduced in Parliament after consulting stakeholders. It felt that concerns of the professional councils such as the Medical Council of India and the Dental Council of India were not adequately addressed. Also, it noted that the powers and functions of the NCHRH and the National Commission on Higher Education and Research (to be established under the Higher Education and Research Bill, 2011 to regulate the higher education sector in the country) were overlapping in many areas. Finally, it also expressed concern over the acute shortage of qualified health workers in the country as well as variations among states and rural and urban areas. As per the 2001 Census, the estimated density of all health workers (qualified and unqualified) is about 20% less than the World Health Organisation’s norm of 2.5 health workers per 1000 population. See here for PRS Standing Committee Summary. Shortfall of health workers in rural areas Public health care in rural areas is provided through a multi-tier network. At the lowest level, there are sub health-centres for every population of 5,000 in the plains and 3,000 in hilly areas. The next level consists of Primary Health Centres (PHCs) for every population of 30,000 in the plains and 20,000 in the hills. Generally, each PHC caters to a cluster of Gram Panchayats. PHCs are required to have one medical officer and 14 other staff, including one Auxiliary Nurse Midwife (ANM). There are Community Health Centres (CHCs) for every population of 1,20,000 in the plains and 80,000 in hilly areas. These sub health centres, PHCs and CHCs are linked to district hospitals. As on March 2011, there are 14,8124 sub health centres, 23,887 PHCs and 4809 CHCs in the country.[i] Sub-Health Centres and Primary Health Centres
Table 1: State-wise comparison of vacancy in PHCs
|
Doctors at PHCs |
ANM at PHCs and Sub-Centres |
|||||
| State | Sanctioned post | Vacancy | % of vacancy | Sanctioned post | Vacancy | % of vacancy |
| Chhattisgarh | 1482 | 1058 | 71 | 6394 | 964 | 15 |
| West Bengal | 1807 | 801 | 44 | 10,356 | NA | 0 |
| Maharashtra | 3618 | 1326 | 37 | 21,122 | 0 | 0 |
| Uttar Pradesh | 4509 | 1648 | 36 | 25,190 | 2726 | 11 |
| Mizoram | 57 | 20 | 35 | 388 | 0 | 0 |
| Madhya Pradesh | 1238 | 424 | 34 | 11,904 | 0 | 0 |
| Gujarat | 1123 | 345 | 31 | 7248 | 817 | 11 |
| Andaman & Nicobar Isld | 40 | 12 | 30 | 214 | 0 | 0 |
| Odisha | 725 | 200 | 28 | 7442 | 0 | 0 |
| Tamil Nadu | 2326 | 622 | 27 | 9910 | 136 | 1 |
| Himachal Pradesh | 582 | 131 | 22 | 2213 | 528 | 24 |
| Uttarakhand | 299 | 65 | 22 | 2077 | 0 | 0 |
| Manipur | 240 | 48 | 20 | 984 | 323 | 33 |
| Haryana | 651 | 121 | 19 | 5420 | 386 | 7 |
| Sikkim | 48 | 9 | 19 | 219 | 0 | 0 |
| Meghalaya | 127 | 23 | 18 | 667 | 0 | 0 |
| Delhi | 22 | 3 | 14 | 43 | 0 | 0 |
| Goa | 46 | 5 | 11 | 260 | 20 | 8 |
| Karnataka | 2310 | 221 | 10 | 11,180 | 0 | 0 |
| Kerala | 1204 | 82 | 7 | 4232 | 59 | 1 |
| Andhra Pradesh | 2424 | 76 | 3 | 24,523 | 2876 | 12 |
| Rajasthan | 1478 | 6 | 0.4 | 14,348 | 0 | 0 |
| Arunachal Pradesh | NA | NA | NA | NA | NA | 0 |
| Assam | NA | NA | NA | NA | NA | 0 |
| Bihar | 2078 | 0 | NA | NA | NA | 0 |
| Chandigarh | 0 | 0 | NA | 17 | 0 | 0 |
| Dadra & Nagar Haveli | 6 | 0 | NA | 40 | 0 | 0 |
| Daman & Diu | 3 | 0 | NA | 26 | 0 | 0 |
| Jammu & Kashmir | 750 | 0 | NA | 2282 | 0 | 0 |
| Jharkhand | 330 | 0 | NA | 4288 | 0 | 0 |
| Lakshadweep | 4 | 0 | NA | NA | NA | 0 |
| Nagaland | NA | NA | NA | NA | NA | 0 |
| Puducherry | 37 | 0 | NA | 72 | 0 | 0 |
| Punjab | 487 | 0 | NA | 4044 | 0 | 0 |
| Tripura | NA | NA | NA | NA | NA | 0 |
| India | 30,051 | 7,246 | 24 | 1,77,103 | 8,835 | 5 |
| Sources: National Rural Health Mission (available here), PRS.Note: The data for all states is as of March 2011 except for some states where data is as of 2010. For doctors, these states are Bihar, UP, Mizoram and Delhi. For ANMs, these states are Odisha and Uttar Pradesh. | ||||||
Community Health Centres
Table 2: Vacancies in CHCs of medical specialists
| Surgeons | Gynaecologists | Physicians | Paediatricians | |
| State |
% of vacancy |
|||
| Andaman & NicobarIsland | 100 | 100 | 100 | 100 |
| Andhra Pradesh | 74 | 0 | 45 | 3 |
| Arunachal Pradesh | NA | NA | NA | NA |
| Assam | NA | NA | NA | NA |
| Bihar | 41 | 44 | 60 | 38 |
| Chandigarh | 50 | 40 | 50 | 100 |
| Chhattisgarh | 85 | 85 | 90 | 84 |
| Dadra & Nagar Haveli | 0 | 0 | 0 | 0 |
| Daman & Diu | 0 | 100 | 0 | 100 |
| Delhi | 0 | 0 | 0 | 0 |
| Goa | 20 | 20 | 67 | 66 |
| Gujarat | 77 | 73 | 0 | 91 |
| Haryana | 71 | 80 | 94 | 85 |
| Himachal Pradesh | NA | NA | NA | NA |
| Jammu & Kashmir | 34 | 34 | 53 | 63 |
| Jharkhand | 45 | 0 | 81 | 61 |
| Karnataka | 33 | NA | NA | NA |
| Kerala | NA | NA | NA | NA |
| Lakshadweep | 0 | 0 | 100 | 0 |
| Madhya Pradesh | 78 | 69 | 76 | 58 |
| Maharashtra | 21 | 0 | 34 | 0 |
| Manipur | 100 | 94 | 94 | 87 |
| Meghalaya | 50 | NA | 100 | 50 |
| Mizoram | NA | NA | NA | NA |
| Nagaland | NA | NA | NA | NA |
| Odisha | 44 | 45 | 62 | 41 |
| Puducherry | 0 | 0 | 100 | NA |
| Punjab | 16 | 36 | 40 | 48 |
| Rajasthan | 57% | 46 | 49 | 24 |
| Sikkim | NA | NA | NA | NA |
| Tamil Nadu | 0 | 0 | 0 | 0 |
| Tripura | NA | NA | NA | NA |
| Uttar Pradesh | NA | NA | NA | NA |
| Uttarakhand | 69 | 63 | 74 | 40 |
| West Bengal | 0 | 57 | 0 | 78 |
| India | 56 | 47 | 59 | 49 |
| Sources: National Rural Health Mission (available here), PRS. | ||||
[i]. “Rural Healthcare System in India”, National Rural Health Mission (available here).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}